Imagine performing delicate neurosurgery guided only by the flickering light of a candle.
Or trying to stitch a wound while relying on the unpredictable midday sun coming through a window.
It sounds like a scene from a medical thriller. But for centuries, this was the precarious reality of the operating room.
We have come a long way from the days of dangerous open flames and the scorching heat of halogen bulbs that left surgeons drenched in sweat. The journey to modern illumination is a fascinating mix of history, physics, and high-tech engineering.
It wasn’t just a quest for brightness. It was a battle to master photobiology—ensuring light interacts safely with living tissue without causing damage or dehydration.
In this post, we’re going to trace the dramatic medical headlamp evolution. We’ll look at how we moved from the rudimentary shadows of the past to the cordless, shadow-free precision of modern LED surgical headlights.
Let’s dive in.
1. Introduction: Illuminating the Operating Room
Here is a simple truth:
Surgical precision is impossible without adequate illumination.
You can have the steadiest hands in the world and the most advanced robotic assistants, but if you can’t see the difference between a nerve and a vessel, the patient is at risk.
Today, we take high-tech “shadowless” operating rooms (ORs) for granted. But the road to the modern LED surgical headlight was paved with trial, error, and a lot of heat.
From Candles to Diodes
The history of medical lighting is a timeline of human ingenuity fighting against darkness.
- 1800s: We relied on weather-dependent windows and dangerous flames.
- 1900s: The electric bulb arrived, bringing light but also intense heat.
- 1960s: Halogen became the standard, improving brightness but tethering surgeons to walls with fiber optic cables.
- 2000s: The LED Revolution changed everything.
The “Great Leap”
The pivotal moment happened in the mid-2000s. This was the era of the “LED Revolution.”
It wasn’t just a small upgrade. It was a total paradigm shift. We moved from hot, yellow, power-hungry bulbs to cool, white, energy-efficient diodes. This shift didn’t just make surgeries brighter; it transformed patient safety and surgeon comfort in ways we are just beginning to fully appreciate.

Alt text: A historical depiction of a 19th-century operating room relying on rudimentary incandescent hanging bulbs.
2. The Dark Ages of Surgery: Pre-20th Century Illumination
If you were a surgeon in 1850, your schedule was dictated by one thing:
The Weather.
Before electricity, operating rooms were architectural marvels designed to capture every ounce of sunlight. They featured massive southeast-facing windows and skylights. Surgeries were strictly scheduled around high noon. If a storm rolled in? You had a problem.
Fire in the Theater
When natural light failed, surgeons turned to fire. Candles, oil lamps, and gas lamps were the standard.
But these came with massive risks:
- Explosions: Ether (an early anesthetic) is highly flammable. Mixing ether fumes with open gas flames was a recipe for disaster.
- Erratic Shadows: A flickering flame casts dancing shadows. If a nurse moved the lamp, the surgeon’s view vanished.
- Hygiene: Oil lamps smoked, creating a less-than-sterile environment.
The Head Mirror (1861)
We can’t talk about history without mentioning the iconic head mirror. Invented in 1861, this concave mirror with a hole in the center allowed a doctor to reflect light from a lamp onto the patient.
It was a rudimentary step toward shadow control, but it required the doctor to hold their head at a precise, rigid angle. It was far from the ergonomic freedom of today’s cordless surgical headlamps.

Alt text: Infographic timeline displaying the evolution of medical headlamps from 1900s incandescent bulbs to modern LED systems.
3. The Age of Heat: Incandescent and Halogen Dominance (1900s-1990s)
As electricity entered the OR in the early 20th century, safety improved. But a new enemy emerged.
Heat.
The Electric Bulb Era
Early incandescent bulbs were safer than gas, but they emitted a yellow-toned light. This made it difficult to distinguish between different types of tissue. Everything looked “muddy.”
The Halogen Standard (1960s)
In the 1960s, Halogen lamps became the gold standard. They used tungsten filaments and halogen gas to create a much brighter, whiter light.
But there was a trade-off.
Halogen vs LED surgery debates often forget how hot halogen actually was. These lamps emitted intense “hot infrared light.”
The “Cooked” Surgeon
Ask any veteran surgeon about the halogen days, and they will tell you about the sweat.
- Surgeon Comfort: To get enough brightness (Lux), halogen lights generated massive amounts of heat. Surgeons would sweat profusely during long procedures, increasing the risk of contamination.
- Tissue Desiccation: The infrared radiation could actually “cook” or dry out the patient’s exposed tissue (tissue desiccation), complicating recovery.
The Tethered Surgeon
To manage this heat, engineers moved the bulb away from the surgeon’s head. They used fiber optic cables to transmit light from a box on the wall to the headset.
The result? The Tether.
Surgeons were physically leashed to a light source.
- Mobility Issues: You couldn’t walk around the table to check a different angle without unhooking or dragging a heavy cable.
- Tripping Hazards: Cables on the floor were a constant safety risk.
- Maintenance: Fiber optic cables are fragile. One heavy cart rolling over a cable could break the glass fibers inside, dimming the light output instantly.
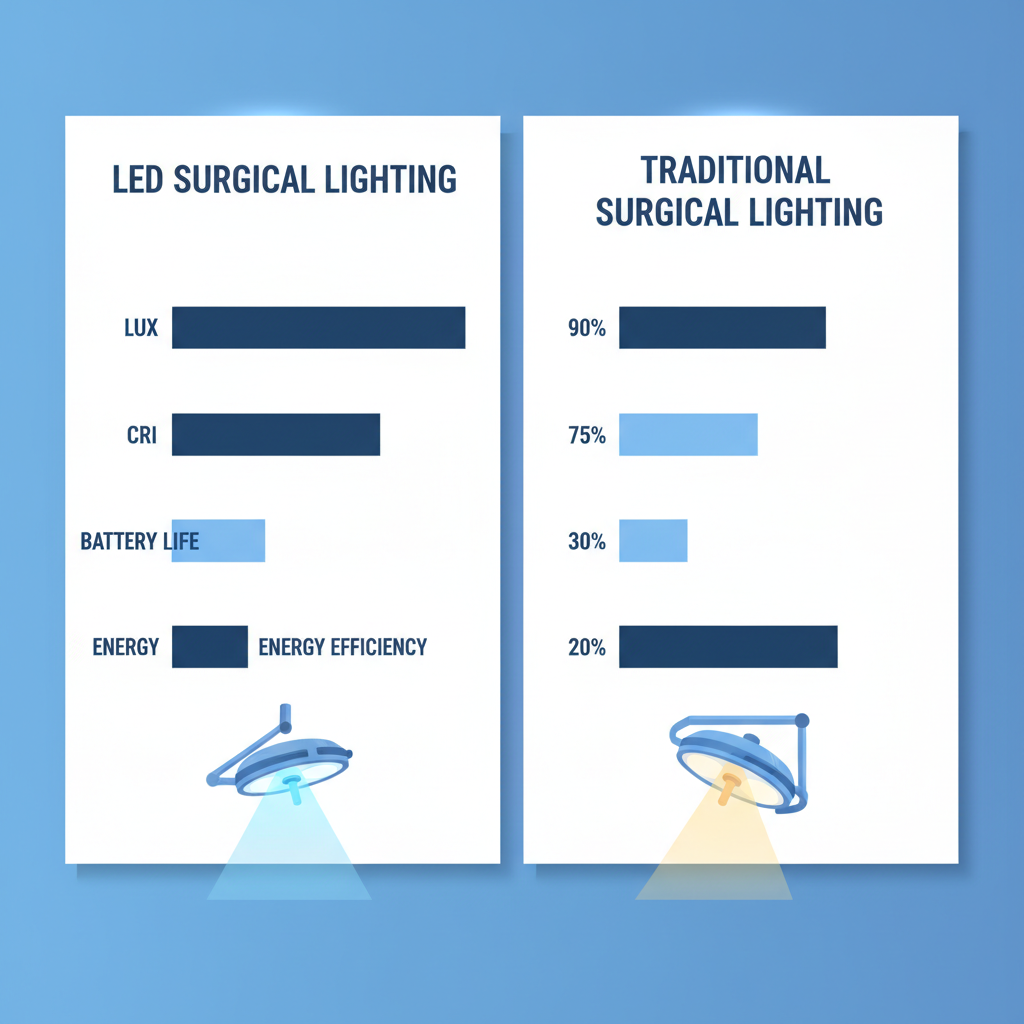
Alt text: Bar chart comparing LED vs Traditional Surgical Lighting across Lux, CRI, Battery Life, and Energy Efficiency.
4. The LED Revolution: A Paradigm Shift in the 2000s
Then came the 2000s.
The introduction of the Light Emitting Diode (LED) into the operating room was the biggest leap in surgical lighting history.
2005: The First Spark
Around 2004-2005, we saw the first LED surgical lights (like the iLED) and the introduction of cordless options like the MedLED “Classic.”
Suddenly, the tether was cut.
The Efficiency Equation
The stats regarding medical headlamp evolution in this era are staggering:
- Energy: LEDs consume up to 70% less energy than halogen systems.
- Longevity: A halogen bulb might last 1,000 hours. A modern medical LED? 50,000 to 60,000+ hours. That is a 50x improvement.
Cooling Down
The biggest win? Thermal Management.LEDs emit minimal heat. A neurosurgeon can work for 12 hours under high-intensity light without breaking a sweat. More importantly, the patient’s tissue remains safe from thermal damage.

Alt text: A modern, compact LED surgical headlamp demonstrating cool white illumination.
5. The Science of Sight: Understanding Uncommon Terms
To understand why High CRI medical lighting is superior, we need to get a little technical. But don’t worry, I’ll keep it simple.
Deciphering Light Quality
It’s not just about brightness (Lux). It’s about quality.
1. CRI (Color Rendering Index)CRI measures how accurate colors look under a light, on a scale of 0-100.
- The Problem: Low CRI lights make red blood and pink tissue look the same shade of brown/grey.
- The Solution: Surgical LEDs require a CRI >90. Even more critical is the R9 value, which specifically measures how well the light renders saturated red. High R9 is crucial for tissue differentiation—distinguishing a healthy artery from a vein or a tumor from a nerve.
2. Lumens per Watt (lm/W)This is “luminous efficacy.” It measures how much light you get for the electricity you use.
- Halogen: Wastes most energy as heat.
- LED: Converts electricity almost entirely to visible light. This allows modern headlamps to hit 225,000 lux (brighter than sunlight) using a tiny battery.
3. Kelvin TemperatureHave you ever noticed how some car headlights are blue and blinding? That’s bad for surgery.
- The Sweet Spot: Medical LEDs aim for “Pure White” (approx. 4,800–6,000 Kelvin).
- Why? It mimics natural daylight at noon. It prevents the yellow cast of halogens (which hides color contrast) and avoids the harsh blue of early LEDs (which causes eye strain).

Alt text: Technical diagram of a surgical headlamp showing internal components including adjustable optics and thermal management systems.
6. Precision Engineering: Shadow Control and Beam Focus
Light is useless if it’s blocked by your own hands.
Banishing Shadows
In the past, overhead lights cast shadows whenever a surgeon leaned over the patient.
Modern headlamps use coaxial illumination. This means the light source is positioned perfectly between the surgeon’s eyes. The light beam follows your line of sight exactly. If you can see it, it’s lit. This eliminates shadows cast by instruments or your own hands.
Deep Cavity Illumination
This is where Beam Angle Adjustment comes into play.
- Surface Work: You need a wide flood of light.
- Deep Work: In neurosurgery or spinal surgery, you are looking down a deep, narrow tube. You need to condense that light into a tight, intense spot.
Modern LED optics allow surgeons to twist the bezel and focus the beam instantly, maintaining uniform brightness (homogeneity) from edge to edge without creating a blinding “hot spot” in the center.

Alt text: Illustration showing how coaxial LED lighting penetrates deep surgical cavities for microsurgery.
7. Unchained: The Rise of Ergonomic, Cordless Headlamps
Remember the “Tethered Surgeon”? That is becoming a thing of the past.
The Weight of Light
Early headlamps were heavy. After an 8-hour shift, surgeons suffered from chronic neck pain. Today, advancements in materials have led to ultra-lightweight designs (**<200g**). We now use “occipital baskets” or cranial support systems that distribute the weight evenly across the skull, rather than letting it hang heavy on the nose or forehead.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}